

How To Set Up A Dental Tray

Diagnosis of impacted third molar should be based on patient complaint, history, physical evaluation and diagnostic exam evaluation.
Preoperative evaluation of the third molar, both clinically and radiographically is an of import stride for the successful and speedy removal. Time spent at this stage is fourth dimension gained. A good periapical radiograph is a must. If required the periapical radiograph should be supplemented with an occlusal X-ray. An OPG or a lateral oblique radiograph should be taken whenever intra oral radiographs are inadequate to provide the necessary information regarding the tooth or side by side structures. However, the sometime lack the details seen in a periapical picture.
PREOPERATIVE PLANNING Aid IN THE Following WAYS
1.It provides a rough gauge of fourth dimension required for the procedure. (Put in extra 15 minutes for any eventuality.)
2.Helps to exclude those cases which are across one'south competence.
3.Look the complications that are likely to occur and get informed consent from the patient
iv.Helps in selection of instruments.
5.Selection of the blazon of anesthesia to be employedwhether local anesthesia or general anesthesia is required. Most patients can tolerate surgery under local anesthesia lasting from 45 minutes to ane hour.
A complete assessment of the possible problems which could exist encountered in the surgical removal of an impacted third tooth and a treatment program can exist formulated but after a careful clinical and radiographic examination of the area.
Clinical Examination
This include (i) History taking (two) Actress oral examination, and (3) Intraoral examination
1. History Taking
Complaints of the patient: Impacted teeth very frequently crusade no symptoms and patients are unaware of its presence until told by the dental practitioner. Symptoms when nowadays are usually related to pericoronitis, which may be either astute or chronic in nature or complaints related to acute pulpitis associated with dental caries. Symptoms associated with other atmospheric condition listed in Chapter 3 nether indications for surgical removal may also exist present.
Medical and dental history: An important part of the interrogation is the medical and dental history of the patient. Advances in modern medicine have resulted in the improved survival of people with pregnant medical conditions. As a result people are living longer and receiving treatment for disorders that were fatal a few years ago. These patients have a relatively loftier run a risk of developing complications from surgical procedures. Hence, information technology is imperative that the dental surgeon be competent to recognize and manage such cases in the safest possible manner. Apart from the fate of the patient, neglect of the medical history can result in unpleasant doctor-legal problems.
There are three basic aspects regarding the dental management of medically compromised patient. The first is to detect such patients. This is a difficult task, specially when there are no significant symptoms or if the patient is uneducated and has no idea about the illness and the drug therapy. However, this does non preclude the responsibility of the dental surgeon in the event any complications occur. Secondly, if the patient is found to have a systemic affliction it is essential to determine the implications of the disease or its treatment on the dental direction. Finally, one time information technology has been decided, information technology and then remains necessary to detect how all-time to deal with the trouble.
In an ordinary dental surgery setting, it is unlikely that the dental surgeon will undertake a full medical examination of the patient prior to any surgical procedures. Instead the operator must rely on a proper medical history that will help to identify those patients with medical weather condition that volition crave precautionary measures. A written questionnaire volition help as a screening measure out to recognize such patients. Alternatively, if the patient is not literate the dental surgeon or the assistant can do a thorough interrogation and the thing entered in the case record. The basic example is as follows:
Medical Evaluation
Date
Delight note to respond the questions correctly. For any clarification contact the dental staff. Your wellness and fitness is of utmost importance to brand certain that the dental treatment you receive volition not affect adversely your full general health.
Proper name, address and Tel. no. of your Medico
Are yous suffering from/ suffered any of the post-obit conditions/ illness?

Exercise you consider yourself to be in the loftier-risk group for HIV/ AIDS/ Hepatitis B

To the all-time of my knowledge, all the preceding answers are true and correct. If I ever take any change in my health, abnormal laboratory test, or if my medication change, I will inform the dentist at the next appointment without fail.

Medical Evaluation Course
A detailed medical history volition help to place medical conditions which contraindicate surgical removal or modify the management of the patient with impacted tooth. A detailed discussion of the medical conditions to be considered is beyond the scope of this chapter.
All the same, the post-obit are the common medical conditions to exist considered which accept pregnant impact in the management of patients with impacted third molar:
ane. Cardiovascular diseases
(a) Hypertension
(b) Infective endocarditis
(c) Ischemic heart disease
(d)Thromboembolic disorders (patientson anticoagulants)
two. Endocrine diseases
(a) Diabetes mellitus
(b) Hyperthyroidism
(c) Adrenal insufficiency
3. Bleeding disorders
4. Respiratory diseases
(a) Bronchial asthma
(b) Chronic obstructive pulmonary affliction (COPD)
5. Liver disease
(a) Chronic alcoholism and Liver cirrhosis
(b) Viral hepatitis
vi. Pregnancy
7. AIDS and HIV infection
8. Prosthetic articulation replacements
9. Neurological Disorders
(a) Epilepsy
(b) Stroke
(c) Parkinson's disease
ten. Patients with organ transplantation
xi. Chronic renal failure
12. Allergy to drugs/ food items
Significance of Medical Evaluation
A proper medical history enables the operator to take the necessary precautions that volition ensure patient'south safety during the dental surgical process. These maybe either i or a combination of the following precautions:
1. Additional investigations: For example clotting screen for those with history of bleeding.
2. Alteration of patient's current medication to facilitate surgery. For example stopping warfarin preoperatively. Such measures must only be taken in consultation with the patient'due south doctor.
3. Administration of preoperative medication: (a) antibiotic encompass, (b) steroid cover, (c) oral sedation
iv.Selection of anesthetic that is safe for the patient
5.Undertaking surgery in a hospital gear up upwards where advisable medical back up is bachelor.
half-dozen.Selection of medication (e.one thousand. antibiotics and analgesics) that is safe for the patient. For instance avert penicillin in those with reported history of allergy.
7.Anticipate and fairly prepare for a potential medical emergency. For case, astute asthmatic set on.
2. Extraoral Examination
The face and neck is examined for signs of swelling or redness of the cheek suggestive of infection. The lower lip is tested for anesthesia or paresthesia. The regional lymph nodes are palpated for enlargement and tenderness.
iii. Intraoral Examination
The following points are noted:
1.Mouth opening: Normal rima oris opening/microsomia/macrosomia/trismus/hypermobility of TM joint/habitual dislocation /fibrosis of mucosa e.g. submucous fibrosis. In retrognathic mandible accessibility to 3rd molar area is restricted, while in prognathic mandible accessibility is meliorate.
ii.Full general examination of oral cavity: Oral mucosa, teeth, oral hygiene.
three.Tertiary molar expanse: State of eruption of tooth, tissue overlying the tooth (os/soft tissue only), signs of pericoronitis.
four.Condition of impacted tooth: Carious or with fillings, internal resorption (not to be mistaken for caries), angulation of tooth, locking of crown of tertiary molar beneath second molar. This is later confirmed with appropriate radiographs.
5.Condition of second molar and first molar: Caries, crown/filling, distal periodontal pocket/resorption of root of second molar, missing 2d molar. Carious second molar or large filling/crown of second tooth is likely to fracture while using leverage in attempting to elevate tertiary molar. The patient has to exist warned of this to avoid unpleasantness subsequently in the event of a mishap.
6. Amount of space available between the distal surface of second molar and the ascending ramus: If the altitude is small, the tooth is less accessible; if large information technology is attainable. In the maxilla the accessibility depends on the relationship of the tooth to the tuberosity. Distal tilting of 2nd molar also decreases accessibility.
vii. Adjacent bone: May be infected along the mesial surface of the tooth and may involve the 2d tooth necessitating its extraction. Infection / osteomyelitis may involve the ramus posterior to the crown particularly in cases of recurrent submasseteric abscess arising in relation to distoangularly impacted third molar.
8. Fracture may complicate the removal of an impacted tertiary molar. When the jaw contains an impacted molar, it is more vulnerable to a blow and ofttimes fractures through an unerupted third tooth catacomb. Afterwards the tooth is removed, the fracture is immobilized in the usual manner. Fracture caused by an attempted surgical removal of 3rd molar should be recognized and a careful record should exist made of it.
9. Pathological complications due to skeletal diseases should be noted. They may increase the danger of fracture as in osteogenesis imperfecta and osteosclerosis. In acromegaly the removal of tooth is difficult because the mandible consists of massive bone. In Paget's disease the molar may be affected by resorption and repair by bone make its removal difficult.
10. Presence of cysts and tumors: Small eruption cysts and large cysts may occur in relation to impacted tooth. Generally they cause displacement of the tooth. Tumors, benign and cancerous may exist found involving the tooth, especially ameloblastoma. Odontomes also may exist found around third molar tooth.
Radiography of Impacted Mandibular 3rd Molar
The purpose of a careful radiological evaluation is to complement the clinical examination by providing additional data virtually the tertiary molar, the related teeth and anatomical features, and the surrounding bone. This is necessary in lodge to make a sound decision about
the proposed surgical procedure, the most advisable location for this to take identify, and to highlight aspects of management which may crave specific mention to the patient.
Moreover, diseases of next soft and difficult tissues may proceed to avant-garde stages without symptoms (e.1000. associated cyst/ tumor), it is important that radiographic evaluation be performed. The well-nigh commonly accepted imaging modality is the intra oral periapical 10-ray and panoramic radiograph. Other imaging techniques may be appropriate if they provide appropriate visualization of the entire tooth and associated structures. However, it must exist kept in mind that radiographs may not provide consummate or authentic information every bit to tooth position.
Most of the local factors causing difficulty in removal of third molar can be diagnosed past careful interpretation of preoperative radiograph.
The following intra oral and extra oral radiographs are required:
1. Periapical radiograph
2. Occlusal X-ray of mandible
3. Lateral oblique view of mandible
four. Orthopantomogram
An important criteria for a expert film is that there should exist a clear superimposition of the buccal and lingual cusps of the second molar upon 1 another in the aforementioned vertical and horizontal airplane which is visualized every bit a typical'enamel cap' appearance of the second tooth.
ane. Periapical radiograph: An ideal periapical 10-ray should include the whole 3rd molar, its investing bone, the anterior border of ramus, the inferior alveolar culvert and the adjacent second molar tooth. An of import criteria for a good flick is that there should be a clear superimposition of the buccal and lingual cusps of the second molar upon one some other in the same vertical and horizontal plane which is visualized every bit a typical 'enamel cap' appearance of the 2nd molar. This tin exist achieved by positioning the X-ray tube in such a way that the central ray will be parallel to the occlusal surface of the 2nd tooth and laissez passer through the distal cusps of the second molar at right angles to the movie packet. In a good motion picture the lateral epitome of the 2d tooth volition be sharp without vertical shortening. In a poor film with wrong angulation, the 'enamel cap' will be absent and in that location will be overlapping of contact points of molars.
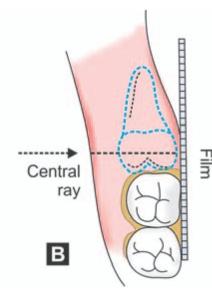
For taking a expert periapical radiograph, the patient is seated with the mouth open, occlusal plane of mandibular teeth horizontal and parallel to the floor. The film is so inserted on the lingual side of the respective third molar with the anterior edge of the picture reaching up to the mesial surface of first molar. In suspected cases of horizontal impaction, the picture should be inserted more posteriorly so that the root apices also will be visualized in the radiograph. A motion picture holder or a direct 'mosquito' hemostat will assistance to grip the picture and position it correctly. The X-ray tube is positioned then that the central ray will be parallel to the occlusal surface of the second molar and pass through the distal cusps of the 2nd molar at right angles to the film packet. Moreover, when viewed from the front the angulation of the central ray should be parallel with the transverse occlusal aeroplane which is commonly at an angle of 3° to 4° above the horizontal plane (Figs six.1 A and B).
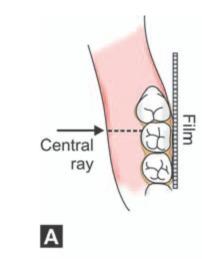
Figs 6.1 A and B: (A) Positioning of periapical film bundle and angulation of key ray in an average case (viewed from higher up), (B) Angulation of the central ray when viewed from the front-the fundamental ray (red pointer) is parallel with the transverse occlusal airplane (greenish line) which is unremarkably at an angle of 3° to 4° above the horizontal plane (blueish dotted line)
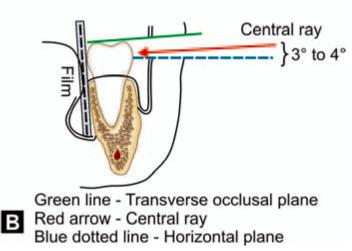
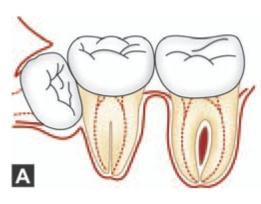
In cases of horizontal impactions, the central ray is directed through the middle of the crown of the impacted molar (Figs vi.2 A and B) and at right angles to the motion picture packet. Lingual tilt or rotation of the second molar if present should be considered while positioning the tube and interpretation of such radiographs.
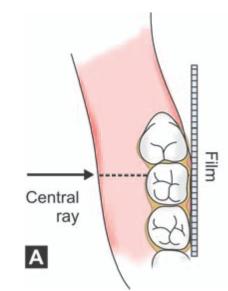
Figs half dozen.2A and B: Location of the picture show and direction of fundamental ray seen from higher up. (A) Average case. Note that central ray is directed along the crown of the second tooth. (B) In case of a horizontal impaction. Note that the cardinal ray is directed through the heart of the crown of the impacted tooth
As stated to a higher place in a practiced picture the lateral image of the 2d tooth will be precipitous without vertical shortening. But in a poor moving-picture show with wrong angulation, the 'enamel cap' will be absent and there will be overlapping of contact points of molars (Figs 6.three A and B). This occurs when the cardinal ray is not parallel to the transverse occlusal plane and if the central ray does not pass at correct angles to the film in the horizontal plane.
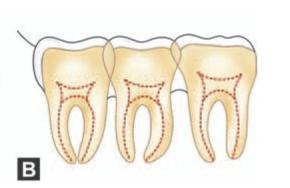
Figs 6.3 Aand B: (A) Schematic diagram showing that when the central ray is non parallel to the transverse occlusal aeroplane the enamel cap of the second molar is absent, (B) If the central ray does not pass at right angles to the film in the horizontal airplane, overlapping of contact points occur
Very oft the correct positioning of periapical film in the 3rd molar region can be hard due to gagging reflex or pain in the floor of the mouth due to abrupt border of the film or difficulty in positioning the 10-ray picture show sufficiently posteriorly. Should these difficulties occur, the resulting moving picture will be far from adequate to yield sufficient data most the impacted molar and surrounding area. Also the narrow viewing field obtained in periapical film has limited diagnostic value. Still, periapical radiographs are more discriminating than OPG and may exist more than helpful in detecting caries, bone top at the level of 2d molar and root profile.
2. Occlusal 10-ray: This will help to confirm the presence of a bucco-lingual human relationship indicated by a periapical 10-ray, and will demonstrate the exact position of the crown of the tooth and the shape of laterally deviated roots.
iii. Lateral oblique view of mandible: At that place is inevitable distortion associated with this radiograph due to the need to rotate the opposite side of the mandible out of the path of the fundamental ray during exposure of the movie. Hence, this is not as useful as a good periapical Xray to assess the local factors causing difficulty in removal. However, this X-ray has a definite role in the following situations:
•When periapical motion-picture show could not exist taken due to retching, trismus or some other cause.
•To provide additional information like vertical height of mandible in the area, amount of os below deeply buried impacted tooth in a thin mandible, existence of pathology in the vicinity like cyst / tumor or double impactions.
Since the introduction of OPG, the indication for the use of extra oral X-ray's is express. Yet, its use may be considered in the absence of OPG.
4.Orthopantomogram (OPG): Recently due to easy availability OPG has replaced the lateral oblique view of mandible. All the data bachelor from a lateral oblique view can exist had from OPG with less distortion (Fig. half-dozen.4). Routine use of OPG is an important accelerate in the accurate localization of impacted teeth
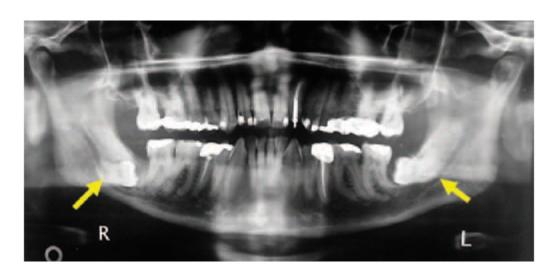
Fig. half-dozen.4: OPG of a 61-twelvemonth-onetime human showing bilaterally impacted tertiary molar with their roots in close relationship to inferior alveolar neurovascular bundle
OPG is considered the aureate standard for surveying the maxilla and mandible for diseases and other pathological conditions in the lateral plane.
Unlike radiographic views helps to identify other conditions affecting the area (Figs 6.five A and B)
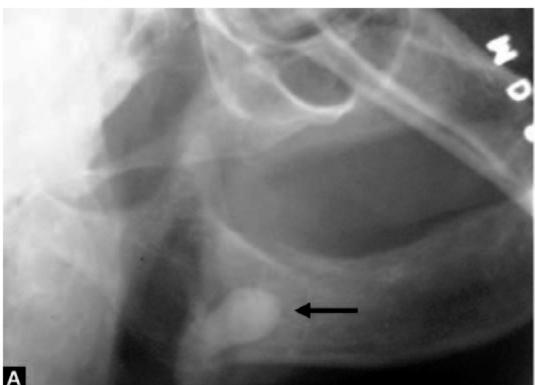
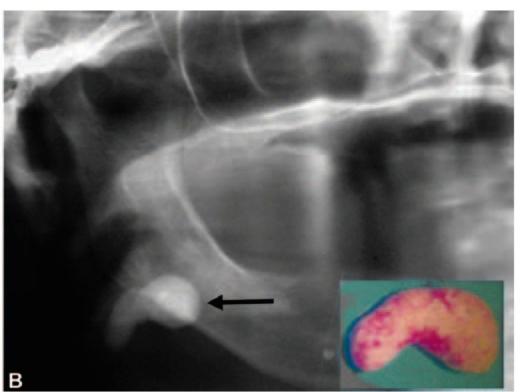
Figs six.5A and B: A 63-year-old lady was referred to the author with a provisional diagnosis of impacted 48 who complained of recurrent pain and swelling of the right side of face with a lateral oblique X-ray of mandible (A) taken by the general dental practitioner (note the dark arrow). Detailed history and findings of clinical examination was suggestive of submandibular calculus. Later an OPG (B) was taken which showed a change in position of the opaque mass which confirmed the final diagnosis of salivary calculus. The calculus was removed (see the inset moving-picture show in figure 'B') under general anesthesia by a submandibular approach
Estimation of Periapical X-ray
The radiograph should be carefully examined in a well lit X-ray foyer. The employ of a skillful hand lens will greatly aid the detection of modest ancillary roots and the relationship of roots to the inferior alveolar culvert.
The post-obit factors are considered while interpreting the radiograph:
a. Access
b. Position and depth of impacted tooth
c. Root pattern of impacted tooth
d. Shape of crown
e. Texture of investing bone
f. Relation to junior alveolar canal
g. Position and root pattern of second tooth.
a. Admission: By noting the inclination of the radioopaque line cast past the external oblique ridge the ease of admission tin be determined. If this line is vertical the admission is poor and if horizontal, access is practiced.
b. Position and depth of impacted tooth: This is adamant by a method described by George Wintertime. In this technique three imaginary lines are drawn on the radiograph. These lines are described as 'white', 'amber' and 'red' lines (Figs 6.6 to 6.ten).

Fig. half dozen.6: White, amber and red lines (Wintertime's State of war lines) marked in the periapical X-ray
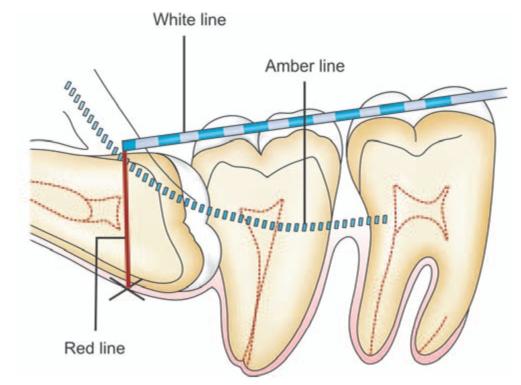
Fig. half dozen.seven: Tracing of War' lines on a horizontally impacted mandibular third tooth. White' line is drawn along the occlusal surface of the erupted mandibular molars and extended posteriorly over the 3rd molar region. 'Amber' line is drawn from the surface of the bone lying distal to the third molar to the crest of the interdental septum betwixt the starting time and second molar. 'Red'line is a perpendicular dropped from the 'amber' line to an imaginary 'bespeak of application' of an lift
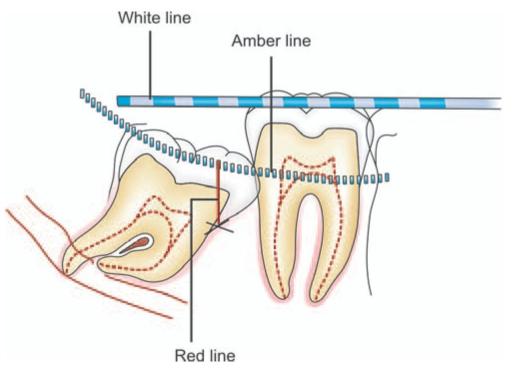
Fig. 6.8: 'War' lines drawn on a mesioangularly impacted mandibular third molar
Fig. vi.ix: 'WAR' lines fatigued on a vertically impacted mandibular third molar. Note that there is no 'red' line fatigued. The point of application of elevator (marked 10 in red color) is at the aforementioned level of 'amber' line at the mesial aspect of the third molar
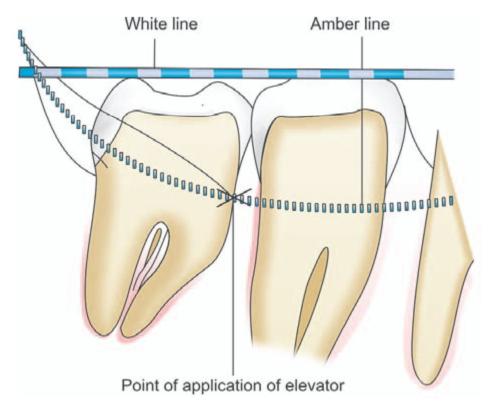
The beginning line or'white' line is drawn along the occlusal surface of the erupted mandibular molars and extended posteriorly over the third molar region. From this the axial inclination or position of impacted tooth can be assessed. For example, the 'white' line will exist parallel to the occlusal surface of a vertically impacted tooth. While in case of a disto-angular impaction, the occlusal surface of the molar and 'white' line are seen to converge every bit if to encounter in front end of the third tooth.
The 'white' line also provides an indication regarding the depth at which the tooth is lying in mandible, when compared to the erupted 2nd molar.
The second imaginary line or 'amber' line is drawn from the surface of the bone lying distal to the third molar to the crest of the interdental septum betwixt the kickoff and second molar. When drawing this line information technology is of import to differentiate between the shadow bandage by the external oblique ridge and that cast past the bone lying distal to the tooth. It is of import to notation that the posterior end of the 'amber' line is drawn on the shadow cast by the os in the retromolar fossa and non that cast past the external oblique ridge which lies above and in forepart of it. The 'amber' line indicates the margin of the alveolar bone enclosing the molar. Hence, when soft tissues are reflected, just that portion of the tooth shown on the picture show to be lying above and in front of the 'amber' line will be visible; while the reminder of the molar volition be encased within the alveolar bone.
Only gilded members can go on reading. Log In or Register to continue

How To Set Up A Dental Tray,
Source: https://pocketdentistry.com/instrument-tray-set-up/
Posted by: harrisonkeing2001.blogspot.com
0 Response to "How To Set Up A Dental Tray"
Post a Comment